A DVT clot sitting silently in your calf can, if it becomes unstable, move through your internal anatomy with surprising speed. Deep vein thrombosis (DVT) and pulmonary embolism (PE) are two stages of the same condition: venous thromboembolism. This occurs when a DVT in the leg leads to a blood clot that travels to the lung circulation, creating a life-threatening blockage [1].
As a vascular specialist, I see many patients who are unaware that a leg issue can affect their breathing. This article explains, step by step, the physiological mechanism underlying this journey, from its initial formation in the lower extremities to its arrival in the pulmonary arteries.
Table of Contents

How a DVT in the Leg Clot Becomes a Lung Clot
A clot forms in a deep leg vein and, if it loses its attachment to the vessel wall, it is swept into the upward flow of venous blood. Once detached, a DVT can travel through the venous system, through the right side of the heart, and into the pulmonary arteries [4]. Because the heart pumps blood directly into the lungs for oxygen, any loose clot fragment in the deep veins is naturally funneled into the lung’s vascular network, where it becomes lodged and blocks blood flow.
Step 1 .. Where and Why DVT Clots Form
The Most Common Location: The Calf
The journey often begins in the lower extremities. Many lower-extremity DVTs begin in the calf veins [2]. The calf muscles act as a pump for the deep veins, but when this pump is inactive, blood can pool and thicken.
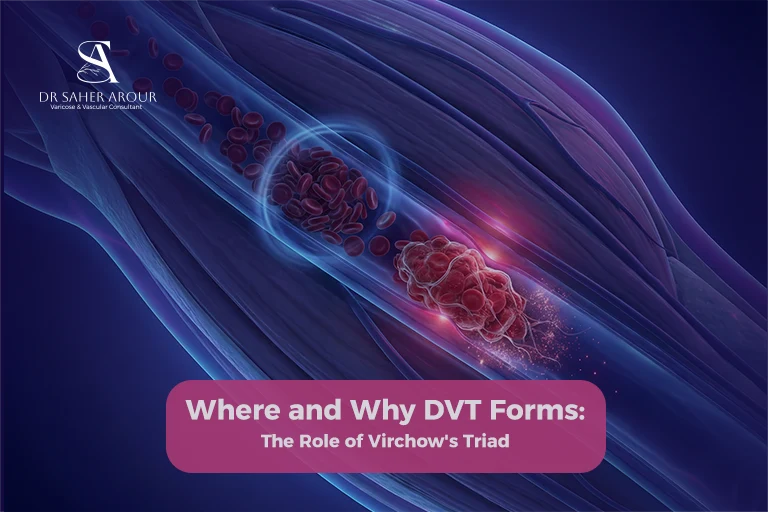
Virchow’s Triad .. Why Blood Clots Form
Vascular surgeons look at three primary factors, known as Virchow’s triad, to understand clot formation. Virchow’s triad includes endothelial or vessel wall injury, stasis or altered flow, and hypercoagulability [3]. Whether due to surgery, long-haul travel, or underlying health conditions, these three factors create the perfect environment for blood to solidify where it shouldn’t.
Step 2 .. What Makes a Clot Detach and Travel
Not All Clots Are Equal
The risk of a clot traveling depends heavily on its stability. A “thrombus” is a clot that remains attached to the vein wall. It only becomes an “embolus” (a traveling clot) when it fragments or completely detaches. This detachment is often triggered by sudden changes in venous pressure or by physical movement after a long period of stasis.
The Role of Clot Age
Fresh clots are typically more gelatinous and fragile, making them more likely to break apart. Over time, the body attempts to “organize” the clot, making it firmer and more adherent to the vein wall. However, during the early stages of formation, the risk of a piece breaking off and starting its journey to the lung is at its highest.
Step 3 .. The Anatomical Journey from Leg to Lung
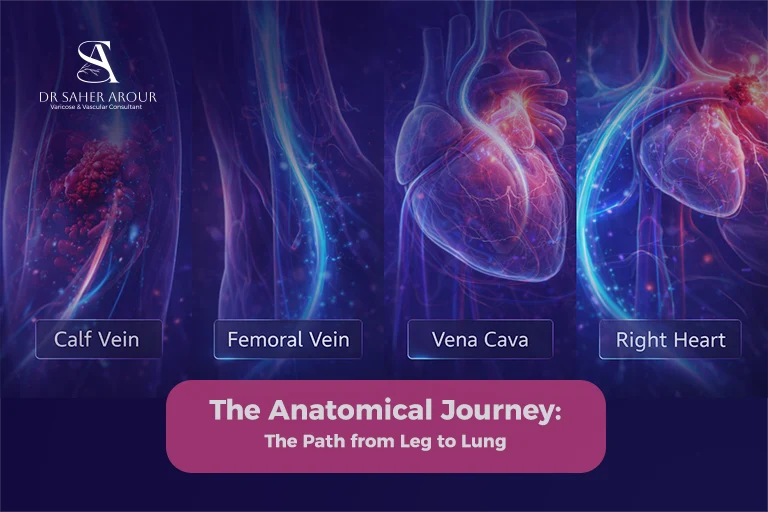
Through the Deep Venous System
Once a fragment breaks free, it enters the “highway” of the deep venous system. It travels from the smaller calf veins into the popliteal vein, then the femoral vein, and finally the iliac veins in the pelvis. All of these eventually lead to the inferior vena cava: the largest vein in the body, which carries deoxygenated blood back to the heart.
Through the Right Heart
The clot enters the right atrium of the heart, passes through the tricuspid valve into the right ventricle, and is then pumped out with significant force. Because the heart’s anatomy is a one-way system, there is no other path for the clot to take but forward into the lungs.
Into the Pulmonary Circulation. Where It Lodges
The clot enters the pulmonary artery, which branches into smaller and smaller vessels within the lung tissue. The clot continues to travel until it reaches a vessel too narrow to pass through. It then wedges itself in place, causing a pulmonary embolism. This blockage prevents blood from reaching the lung tissue to pick up oxygen, which is why breathlessness is a primary symptom.
Comparing PE Risk Based on Clot Characteristics
Not every DVT carries the same probability of traveling to the lungs. The following table summarizes the risks based on evidence-backed clinical factors:
| Clot Feature | Location/Type | PE Risk Level | Medical Evidence Summary |
| Location | Proximal (Thigh/Pelvis) | High (Up to 50%) | Confers up to 50% risk if untreated [5] |
| Location | Distal (Calf only) | Lower | Less likely to be a source of large emboli [8] |
| Ultrasound View | Free-floating thrombus | Very High (77%) | 77% risk vs 23% for non-floating clots [6] |
| Health Status | Active Cancer | Increased | 4- to 7-fold increased VTE risk [7] |
Why Some DVTs Cause PE and Others Don’t
Factors That Increase PE Risk from DVT
- Proximal location: DVT in the popliteal, femoral, or iliac veins carries a substantially higher PE risk than distal (calf) DVT. Proximal DVT confers up to a 50% risk of pulmonary embolism if left untreated [5].
- Free-floating thrombus: A free-floating DVT visible on ultrasound is associated with a higher risk of PE compared to a non-floating thrombus: 77% vs. 23% [6].
- Active cancer: This is a major risk factor for VTE overall, with a 4- to 7-fold increased risk of developing the disease [7].
Protective Factors That Reduce PE Risk
- Distal-only (calf) DVT: These clots are smaller and less likely to be a source of large, dangerous emboli [8].
- Early anticoagulation: This is the cornerstone of treatment. Anticoagulation aims to prevent PE and stop existing clots from growing [9].
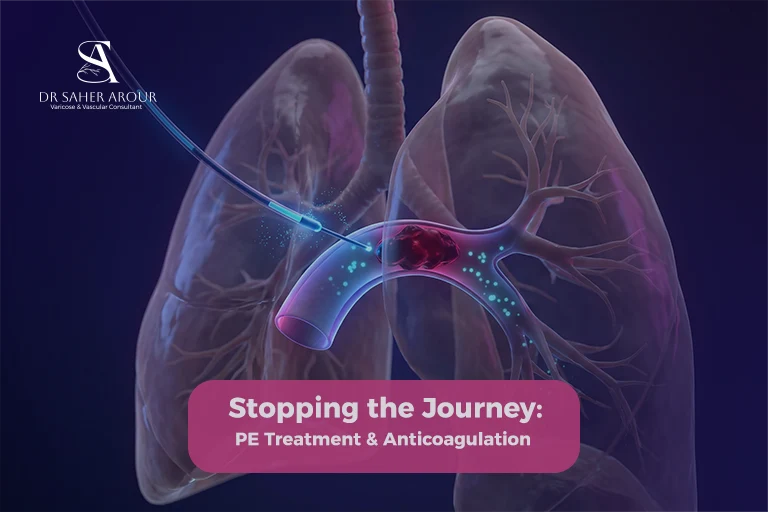
How Treatment Stops the Journey
Anticoagulation .. Stabilising the Clot
It is a common misconception that “blood thinners” dissolve clots. In reality, anticoagulants do not dissolve a clot: they prevent new clots and stop existing ones from growing larger [10]. This allows the body’s natural processes to stabilize and eventually reabsorb the clot over time. For more details, see our complete guide to pulmonary embolism and DVT treatment.
Catheter-Based Treatment .. When Anticoagulation Is Not Enough
In most patients, medication alone is preferred. However, for selected severe cases of PE or extensive DVT, interventional procedures are used [14]. Dr. Saher Arour’s catheter-based PE treatment.. which received a Dubai innovation award.. allows for the mechanical removal of the clot in emergencies where the heart is under significant strain.
DVT Symptoms You Must Not Ignore
- Swelling in one leg only: This is a classic sign of DVT [11].
- The PE Emergency: If breathlessness or chest pain accompanies leg swelling, this is a PE emergency and requires immediate medical intervention [11].
References
- [1] Centers for Disease Control and Prevention: DVT Basics
- [2] Circulation: DVT and PE Review
- [3] StatPearls: Virchow Triad
- [4] Yale Medicine: How PE Occurs
- [5] Cleveland Clinic: Proximal DVT Risks
- [6] PubMed: FFT and PE Incidence
- [7] PMC: Cancer as a Risk Factor for VTE
- [8] Merck Manual: Distal vs Proximal DVT
- [9] StatPearls: DVT Treatment Cornerstone
- [10] AHA: How Anticoagulants Work
- [11] NHS: DVT and PE Symptoms
- [12] StatPearls: Early Ambulation in DVT
- [13] NHLBI: PE Symptom Onset
- [14] CHEST Guideline 2021: Antithrombotic Therapy